| |
If
You're Considering Breast Reconstruction...
Reconstruction
of a breast that has been removed due to cancer or other disease
is one of the most rewarding surgical procedures available today.
New medical techniques and devices have made it possible for surgeons
to create a breast that can come close in form and appearance to
matching a natural breast. Frequently, reconstruction is possible
immediately following breast removal (mastectomy), so the patient
wakes up with a breast mound already in place, having been spared
the experience of seeing herself with no breast at all.
But
bear in mind, post-mastectomy breast reconstruction is not
a simple procedure. There are often many options to consider
as you and your doctor explore what's best for you.
The
Best Candidates For Breast Reconstruction
Most
mastectomy patients are medically appropriate for reconstruction,
many at the same time that the breast is removed. The best
candidates, however, are women whose cancer, as far as can
be determined, seems to have been eliminated by mastectomy.Still,
there are legitimate reasons to wait. Many women aren't comfortable
weighing all the options while they're struggling to cope with
a diagnosis of cancer. Others simply don't want to have any
more surgery than is absolutely necessary. Some patients may
be advised by their surgeons to wait, particularly if the breast
is being rebuilt in a more complicated procedure using flaps
of skin and underlying tissue. Women with other health conditions,
such as obesity, high blood pressure, or smoking, may also
be advised to wait.
In
any case, being informed of your reconstruction options before
surgery can help you prepare for a mastectomy with a more positive
outlook for the future.
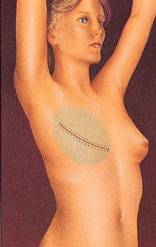
Skin
expansion
The most common technique
combines skin expansion and subsequent insertion of an implant.Following
mastectomy, your surgeon will insert a balloon expander beneath
your skin and chest muscle. Through a tiny valve mechanism
buried beneath the skin, he or she will periodically inject
a salt-water solution to gradually fill the expander over several
weeks or months. After the skin over the breast area has stretched
enough, the expander may be removed in a second operation and
a more permanent implant will be inserted. Some expanders are
designed to be left in place as the final implant. The nipple
and the dark skin surrounding it, called the areola, are reconstructed
in a subsequent procedure.Some patients do not require preliminary
tissue expansion before receiving an implant. For these women,
the surgeon will proceed with inserting an implant as the first
step.
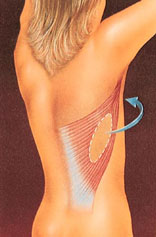
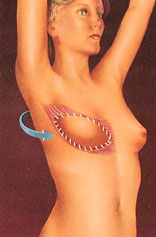
Flap reconstruction
An alternative approach
to implant reconstruction involves creation of a skin flap
using tissue taken from other parts of the body, such as the
back, abdomen, or buttocks.In one type of flap surgery, the
tissue remains attached to its original site, retaining its
blood supply. The flap, consisting of the skin, fat, and muscle
with its blood supply, are tunneled beneath the skin to the
chest, creating a pocket for an implant or, in some cases,
creating the breast mound itself, without need for an implant
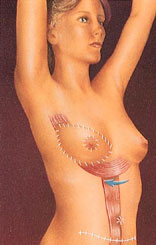
.Another
flap technique uses tissue that is surgically removed from
the abdomen, thighs, or buttocks and then transplanted to the
chest by reconnecting the blood vessels to new ones in that
region. This procedure requires the skills of a plastic surgeon
who is experienced in microvascular surgery as well.
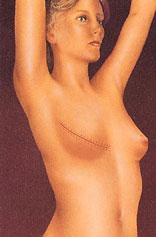
Regardless
of whether the tissue is tunneled beneath the skin on a pedicle
or transplanted to the chest as a microvascular flap, this
type of surgery is more complex than skin expansion. Scars
will be left at both the tissue donor site and at the reconstructed
breast, and recovery will take longer than with an implant.
On the other hand, when the breast is reconstructed entirely
with your own tissue, the results are generally more natural
and there are no concerns about a silicone implant. In some
cases, you may have the added benefit of a improved abdominal
contour.
Follow-up
procedures. Most breast reconstruction involves
a series of procedures that occur over time. Usually, the
initial reconstructive operation is the most complex. Follow-up
surgery may be required to replace a tissue expander with
an implant or to reconstruct the nipple and the areola. Many
surgeons recommend an additional operation to enlarge, reduce,
or lift the natural breast to match the reconstructed breast.
But keep in mind, this procedure may leave scars on an otherwise
normal breast and may not be covered by insurance
|